What Is an Impacted Canine?
An impacted canine is a permanent canine tooth that has failed to erupt into its correct position in the dental arch by the expected age (typically age 12 to 14 in girls and 13 to 15 in boys).
The most common impaction site is the upper canines (about 2 percent of the population), with the canine displaced palatally (toward the roof of the mouth, in roughly two-thirds of cases) or buccally (toward the cheek, in the remaining third). Lower-canine impaction is much rarer.
The clinical concern is not aesthetic. An impacted canine that is left in place tends to drift over years, resorbing the roots of the adjacent lateral incisor or first premolar. Permanent root loss in those neighbors is the worst-case outcome, and it is silent and progressive without 3D imaging.
Limestone Hills screens for canine impaction at every Phase 1 evaluation around age 9 to 11 specifically because catching the problem before the canine is fully impacted dramatically simplifies treatment and reduces the risk of root resorption damage.
Why Canine Teeth Are Worth Saving
Modern orthodontics nearly always favors saving the impacted canine over removing it for two structural reasons. The canine is the longest-rooted tooth in the mouth, with a deep bony attachment that anchors the corner of the arch and supports the lip and cheek architecture.
Replacing it cosmetically with a premolar substitution or a dental implant produces an arch that is mechanically weaker and aesthetically asymmetric in roughly half of cases (the canine eminence visible at the corner of the smile cannot be reproduced by either substitute).
The canine also leads occlusion in lateral movements (canine guidance), distributing chewing forces across the arch in a way that protects the molars from cusp-tip wear. Premolar substitution shifts that load onto teeth the dentition was not designed to bear in lateral function.
Patients in their 50s and 60s whose canines were extracted in adolescence often present with asymmetric posterior wear and TMJ symptoms that trace back to the missing canine guidance.
The Limestone Hills Approach to Impacted Canines
Three-dimensional imaging first. An impacted canine cannot be treated correctly without CBCT. On a 2D panoramic x-ray, a canine trapped in the palate looks nearly identical to a canine trapped in the buccal (cheek) side, and the treatment is different. Once position is clear, Dr. Viecilli works with the oral surgeon on exposure and bonds a chain to the tooth, then pulls it into the arch along a biomechanically sensible path. Recovery, root length, and adjacent-tooth damage depend on the approach chosen before the surgery starts, which is why the imaging and planning step matters more than the surgical step.
The practical sequence runs about 9 to 18 months depending on canine position.
CBCT planning at the consultation, surgical exposure with a periodontist or oral surgeon (typically a 30-minute outpatient procedure under local anesthesia), and orthodontic traction during comprehensive braces or aligner treatment that brings the canine through the bone and into its correct position.
TADs (temporary anchorage devices) are used routinely as the traction anchor so the rest of the dentition is not dragged toward the impaction site during the long pull-down phase.
Expose-and-Bond vs. Premolar Substitution
The decision between expose-and-bring-down (preserve the canine) and extract-and-substitute (replace with a premolar or implant) is made on three findings from the CBCT scan:
Early Detection: The Age 9–10 Window
The single most consequential intervention in canine-impaction management is early detection. By age 9 or 10, panoramic and CBCT imaging show the path the canine is tracking through the alveolus toward the arch. Three interventions during the active growth window (ages 9 to 12) can each redirect a canine that is heading toward impaction:
Limestone Hills evaluates every Phase 1 patient for canine eruption pathway specifically because the cost-benefit math favors early intervention by a wide margin: a 3-month deciduous-canine extraction at age 10 is incomparably simpler than a 12 to 18 month surgical-exposure-and-traction sequence at age 14.
What Happens If an Impacted Canine Is Not Treated
Left untreated, an impacted canine carries three structural risks that compound over time:
The Impacted Canine Treatment Process at Limestone Hills
CBCT Localization
3D imaging determines the exact position, angulation, depth, and relationship to adjacent roots. This guides the surgical approach and the direction of orthodontic traction.
Create Space
Braces are placed and the teeth are aligned to create a gap in the arch where the canine belongs. If the arch is narrow, palatal expansion may be needed first. The baby canine is extracted if still present.
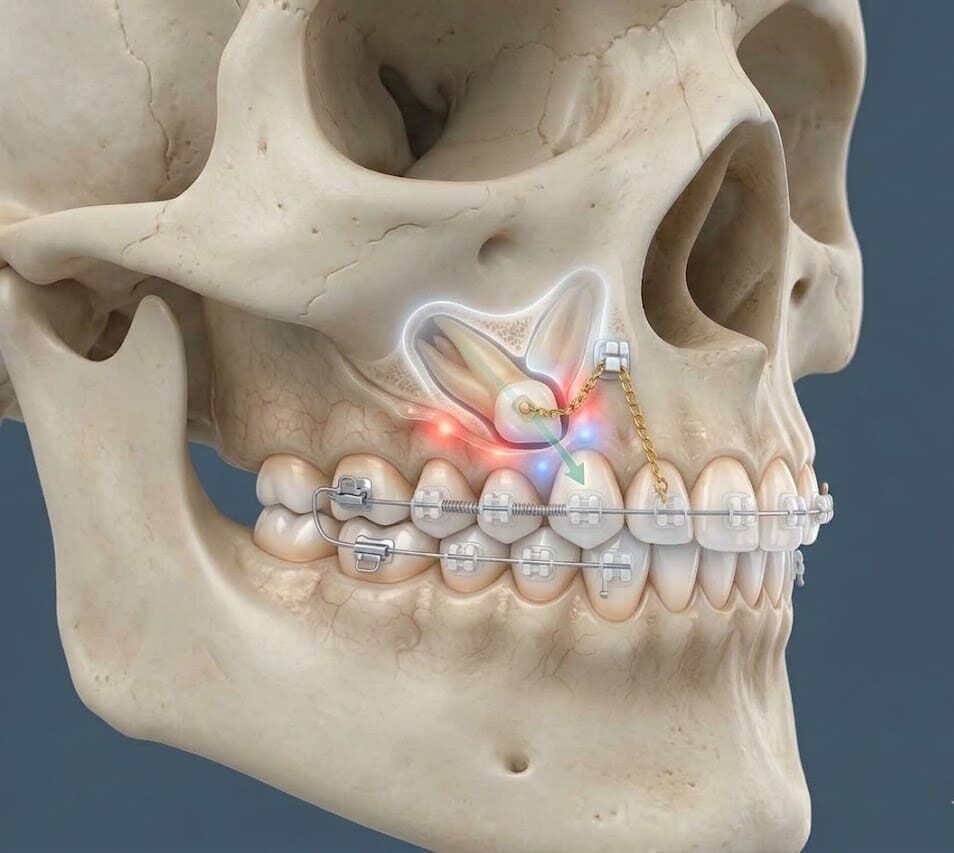
Surgical Exposure
An oral surgeon lifts the gum tissue, removes any overlying bone, and bonds an orthodontic bracket with a small chain onto the impacted canine. Closed technique (gum replaced) or open technique (gum left open) is chosen based on the tooth’s position. Takes approximately 1 hour under local anesthesia.
Orthodontic Traction
Dr. Viecilli uses the chain to apply light, slow traction. Gradually guiding the canine through the bone and into its correct position over 6–12 months. Force must be light to avoid ankylosis (tooth fusing to bone) or root resorption.
Final Alignment
Once the canine has erupted into the arch, comprehensive braces fine-tune its position, establish proper canine guidance, and align the rest of the teeth. Total treatment: 18–30 months.
Why Limestone Hills Handles Impacted Canines Carefully
Three points distinguish the Limestone Hills approach to impacted canines from a generic surgical-orthodontic referral:
Treatment Timeline
| Stage | Duration | What Happens |
|---|---|---|
| Screening & imaging | 1–2 visits | Panorex, CBCT 3D localization |
| Interceptive (ages 10–11) |
6–12 months
|
Baby canine extraction, monitor eruption
|
| Space creation |
4–8 months
|
Braces, expansion if indicated
|
| Surgical exposure |
1 day procedure
|
Oral surgeon exposes and bonds bracket
|
| Traction + alignment |
12–18 months
|
Light traction to guide canine into arch
|
| Detailing & retention |
3–6 months
|
Establish canine guidance, retainers
|
What to Expect at Your Consultation
Before & After


Crowding: Invisalign/Clear Aligners


Deep Overbite: Braces with Bite-Pads
See more impacted canine cases in our treated cases gallery.
How Much Does Impacted Canine Treatment Cost?
The practice coordinates directly with the surgeon for scheduling and insurance pre-authorization. Most dental insurance covers both the orthodontic treatment and the surgical exposure when medical necessity is documented (impacted tooth, risk of root resorption).
Insurance & Financing
Most PPO orthodontic plans cover the orthodontic component (traction, comprehensive treatment); the exposure surgical fee is billed by the partnering periodontist or oral surgeon and is often covered separately under medical insurance. The free CBCT scan at consultation is included.
Common Appliances Used at Limestone Hills
Guiding an impacted canine into position requires fixed braces to hold space open and direct the tooth’s path of eruption over 12 to 18 months; when the anchorage demands of the case are high, temporary anchorage devices give Dr. Viecilli precise control without relying on patient cooperation.