
What Is Reverse-Pull Headgear (a Facemask)?

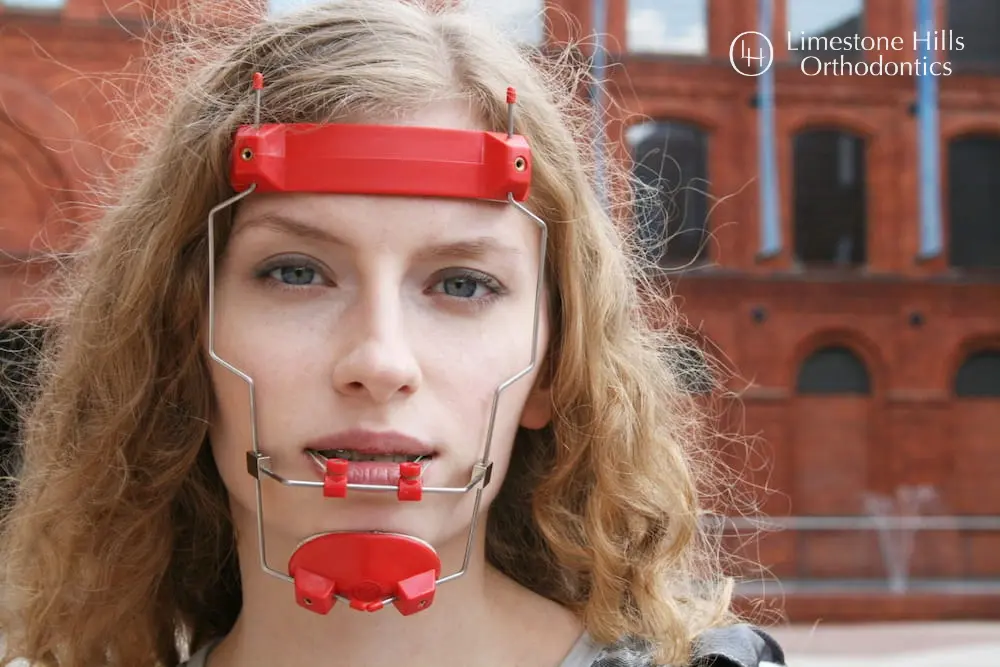
Reverse-pull headgear. Often called a protraction facemask. Is an orthopedic appliance that gently pulls the upper jaw forward to correct an underbite (Class III malocclusion). A soft-padded frame rests on the forehead and chin, and light elastics run from hooks on a palatal expander inside the mouth to the outer frame.
The elastic force coaxes forward growth of the maxilla (upper jaw and midface), not just the teeth.
Unlike traditional “bird cage” headgear. The older appliance pushes the upper jaw backward. A reverse-pull facemask works in the opposite direction. Push-back headgear is rarely used in modern Phase 1 treatment; the facemask has replaced it as the orthopedic tool of choice for skeletal underbite in growing children.
Most Limestone Hills Orthodontics headgear patients are young children whose CBCT scan shows a true Class III skeletal pattern that will worsen without intervention during active jaw growth.
Timing is everything. Between roughly ages 7 and 10, the maxillary sutures are still open and responsive to orthopedic force. After that window, the bony seams that allow the upper jaw to move forward begin to consolidate, and orthodontic tools alone can no longer deliver true skeletal change.
This is why the American Association of Orthodontists recommends a first orthodontic evaluation by age 7. And why Limestone Hills Orthodontics screens every new young patient in Austin for early signs of Class III growth.
When an Austin Child Needs a Facemask
At Limestone Hills Orthodontics, reverse-pull headgear is recommended only when the diagnostic records show a clear skeletal (not purely dental) underbite in a child still in active growth. Dr. Viecilli evaluates the following on 3D CBCT imaging and clinical exam:

Skeletal Underbite (Class III Malocclusion)
The upper jaw sits too far back relative to the lower jaw, so the lower front teeth bite in front of the upper front teeth. Left untreated during active growth, the pattern tends to worsen through adolescence as the lower jaw continues to grow past the upper.
Many untreated Class III cases eventually require orthognathic (jaw) surgery in adulthood. A well-timed facemask during childhood can eliminate or dramatically reduce that risk.
Midface Deficiency
The middle third of the face. Cheekbones, the upper lip base, and the area beneath the eyes. Appears flat or recessed. This is the hallmark of an underdeveloped maxilla. A facemask does not just move teeth: it stimulates forward growth of the entire maxillary complex, which improves both bite and facial balance.
Anterior Crossbite From a Skeletal Cause
One or more upper front teeth bite behind the lower. When the cause is skeletal (not just a tipped tooth), braces alone mask the problem without addressing the underlying jaw position. A facemask combined with expansion treats the root cause.
Family History of Underbite
Class III patterns carry a strong genetic signal. If a parent, grandparent, or sibling has an underbite or had jaw surgery, Limestone Hills Orthodontics urges early evaluation. Ideally around age 7. So the narrow growth window is not missed.
This is especially important for families across Austin and the surrounding Austin and the surrounding communities communities who may not realize how early the Class III treatment window closes.
Correcting a Class III Skeletal Underbite
Class III correction with a facemask is an orthopedic procedure, not simply an orthodontic one. The goal is to remodel the position of the upper jaw itself. The maxilla. During the limited years when that bone can still be moved forward. This is fundamentally different from later teen or adult orthodontics, where brackets and elastics reposition teeth within jaws that are already mature.
Why Limestone Hills Orthodontics Treats Phase 1 Class III Cases
Dr. Viecilli views Phase 1 intervention as appropriate for a narrow set of structural problems. True skeletal underbites, multi-tooth crossbites with functional shift, severely constricted palates, and severe crowding that would trap adult canines.
Cosmetic crowding that growth is likely to resolve on its own is not a Phase 1 indication. When a child in Austin does show a true Class III pattern, however, the cost of waiting is high: the difference between a 3–6 month facemask phase at age 8 and a two-jaw surgery at age 18.
A facemask cannot reverse a skeletal underbite that has already settled into an adult jaw. Once the maxillary sutures finish fusing. Usually in the mid-teens for boys, a bit earlier for girls. The forces a facemask delivers can no longer separate the bony seams needed for forward movement.
For teens whose growth window has closed, Limestone Hills Orthodontics coordinates alternative pathways: MARPE (Miniscrew-Assisted Rapid Palatal Expansion) for transverse correction in adults, Class III elastics with braces for camouflage of mild-to-moderate cases, and orthognathic surgery for severe skeletal discrepancies.
The Limestone Hills Orthodontics Phase 1 Protocol
Phase 1 Class III treatment at Limestone Hills Orthodontics is sequenced, not improvised. The goal in the Phase 1 growth window (approximately around age 7) is to correct the skeletal relationship once, then monitor growth until the adult teeth are ready for any finishing work.
Free Consultation and Diagnostic Imaging
Dr. Viecilli evaluates the child’s bite, facial balance, and airway, and takes a 3D CBCT scan (included at no cost). The scan confirms whether the underbite is skeletal, dental, or both, shows the maturity of the maxillary sutures, and reveals how much forward growth potential remains. Parents see the 3D images on-screen and receive a clear plan.
Rapid Palatal Expansion First
Most Class III children also have a narrow upper jaw. Expansion is the first step, because widening the palate simultaneously loosens the maxillary sutures. This primes the bone to respond to the facemask that follows.
Limestone Hills Orthodontics uses a slim, molar-only rapid palatal expander custom-fit to the child’s jaw. Active expansion typically finishes within 10 to 14 days.
Facemask Fitted and Elastics Connected
As soon as active expansion is complete, the facemask is fitted. Elastic bands connect from hooks on the expander inside the mouth to the facemask frame outside. Dr. Viecilli adjusts the force level and direction and shows the child and parent how to attach and remove the elastics at home. Fresh elastics go on each morning.
Month 1 – Full-Time Wear
This is the most productive month of the entire protocol. The maxillary sutures are still loose from expansion and will not stay open indefinitely. Within 4 to 6 weeks, they begin to re-consolidate. Limestone Hills Orthodontics recommends wearing the facemask as much as possible during this window: at home, during homework, and during sleep.
The appliance comes off only for meals, brushing, and active sports. Applying full-time force while the sutures are still mobile produces meaningfully more skeletal change (forward jaw movement) than the same force applied once the bone has settled.
Months 2–3 – Evening and Overnight Wear
As the sutures stabilize, wear time tapers to roughly 14 hours per day. Evenings, homework time, and overnight. School hours and sports days no longer require the facemask. Check-ups every 4 to 6 weeks let Dr. Viecilli monitor forward movement and fine-tune elastic force.
Re-Evaluation After Approximately 3 Months
A follow-up CBCT or clinical exam confirms the skeletal correction. Most patients discontinue the facemask at this point and transition either to watchful monitoring (if the adult teeth have not yet erupted) or to Phase 1 braces to fine-tune alignment.
The palatal expander is typically left in place for 4 to 6 months after initial placement so the widened palate can stabilize.
Why the Expander and Facemask Work Together
Expansion and facemask therapy are not two separate treatments. They are one coordinated orthopedic procedure.
Limestone Hills Orthodontics’s palatal expander page explains the expansion side in detail, but the short version matters here: rapid palatal expansion disrupts the circummaxillary sutures that connect the upper jaw to the rest of the skull. For 4 to 6 weeks afterward, those sutures are in a state of active remodeling.
That remodeling window is exactly when the facemask delivers the most skeletal correction per ounce of force. The maxilla can be drawn forward through sutures that are, temporarily, still flexible. Outside that window, the same elastics mostly move teeth rather than bone. This is why Class III camouflage treatment in older teens looks very different from Phase 1 correction in an 8-year-old.
This is also why Limestone Hills Orthodontics does not postpone facemask placement after expansion is complete. Waiting a few months for convenience quietly trades skeletal correction for dental compensation.
What to Expect Day to Day
First Few Days
Most children feel mild pressure on the forehead and chin for the first 2 to 3 days. Similar to the sensation of wearing a new helmet or breaking in a pair of shoes. The pressure is not sharp pain; it is the feeling of gentle, continuous forward pull. Padding adjustments at the first check-up resolve any specific comfort issues.
Sleep
Sleeping in the facemask takes a few nights to get used to. Back sleeping works best, and a slightly flatter pillow often helps. Most families report the child settles into a routine by the end of the first week.
Eating and Brushing
The facemask comes off for every meal and every brushing session. The palatal expander stays in. Regular hygiene. Fluoride toothpaste, gentle brushing around the expander, and water-flossing as needed. Is all that is required. No special products.
Speech
Speech is not affected by the facemask itself, because the frame sits entirely outside the mouth. The palatal expander inside may temporarily affect “s” and “sh” sounds for a few days; most children adapt within a week.
Sports and School
During Month 1 full-time wear, the facemask comes off for active sports and can come off for school if the child prefers. After Month 1, it is worn only at home. Because the active phase is short, most Austin families find the at-home-only schedule workable alongside schoolwork and activities.
Visible Results
Parents often notice improved facial profile within the first month. A fuller upper lip, more forward cheek projection, and a bite that is beginning to look balanced at rest. Because the correction is skeletal, those changes hold as the face continues to grow.
Headgear for Adults – Why Limestone Hills Orthodontics Rarely Recommends It
Reverse-pull headgear depends on open maxillary sutures for its effect. Once the sutures have fully fused. Generally by the late teens. A facemask can no longer deliver meaningful skeletal correction, regardless of how long it is worn. For adults with a Class III pattern, Limestone Hills Orthodontics evaluates:
Traditional “pull-back” cervical headgear (sometimes called “bird cage” headgear) for Class II correction is likewise rarely used at Limestone Hills Orthodontics today. Modern Class II mechanics – Herbst, MARA, Forsus, Carriere, and Class II elastics. Typically, achieve the same correction without headgear strap compliance issues.
Each of those alternatives is discussed with families when a Class II growth pattern is diagnosed.
How Much Does Reverse-Pull Headgear Cost in Austin?

Included With a Phase 1 Treatment Plan
No separate charge for the facemask appliance or elastics.
The reverse-pull facemask is included as part of a comprehensive Phase 1 orthodontic treatment plan at Limestone Hills Orthodontics. The total Phase 1 fee. This typically bundles expansion, facemask therapy, monitoring visits, and any Phase 1 braces. Depends on the complexity of the case and is quoted in writing at the free consultation.
Many dental insurance plans cover a portion of Phase 1 interceptive orthodontic treatment. Limestone Hills Orthodontics accepts most PPO plans and verifies benefits before treatment begins. For families without orthodontic insurance, or for the portion that insurance does not cover, the following financing options are available:
For a personalized estimate, book a free consultation. The visit includes a 3D CBCT scan, a bite evaluation, and a full written cost breakdown at no charge. See the insurance guide for coverage verification, and the community discounts page for military, teacher, first-responder, and family discounts, which also apply to comprehensive Phase 1 plans.
Frequently Asked Questions
What is reverse-pull headgear?
It is most effective in children ages 7 to 10, before the maxillary sutures begin to fuse.
How long does a child need to wear a facemask?
This post-expansion protocol takes advantage of the window when the maxillary sutures are still loose and most responsive to forward force, producing a greater share of skeletal (as opposed to dental) correction.
What is the best age for reverse-pull headgear?
The American Association of Orthodontists recommends a first orthodontic evaluation by age 7, which is early enough to identify underbite and begin treatment during the optimal growth window. Children who present at Limestone Hills Orthodontics closer to age 10 or 11 can often still be treated, but the window narrows quickly.
Does reverse-pull headgear hurt?
Can a teen or adult wear a facemask?
How is this different from “regular” (push-back) headgear?
Most Class II cases at Limestone Hills Orthodontics today are treated with functional appliances, elastics, or clear aligner mechanics rather than push-back headgear.